Smart Diagnostics for Low Resource Settings | TU Delft Repositories
ongoing
Master thesis by Merlijn Sluiter
Check out the project video here!
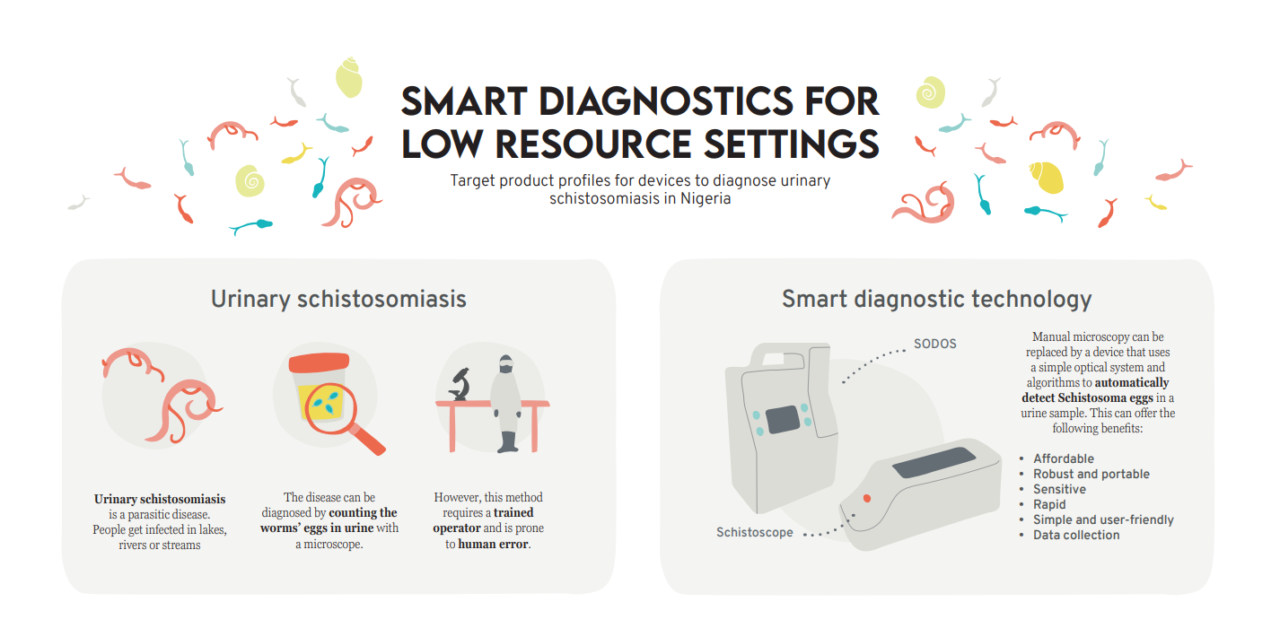
Urinary schistosomiasis is a neglected tropical disease caused by the Schistosoma haematobium parasite. People can get infected when they get into contact with contaminated fresh water. The disease is most prevalent amongst children, farmers and rural communities in Sub-Saharan Africa. Currently, the disease is diagnosed by microscopic egg count in laboratories. However, there are limitations to use of this method in low resource settings. At Delft University of Technology, smart diagnostics are under development that allow diagnosis of urinary schistosomiasis without microscope. However, the user and diagnostic setting for these tests has not been specified yet. The goal of this project is to combine gaps in the healthcare system and the needs of stakeholders with technological possibilities into a target product profile for a diagnostic device for urinary schistosomiasis for specific use case scenarios. This project takes Nigeria as study field. There are two optical diagnostic methods under development, which combine a simple optical system with an algorithm to automatically detect S. haematobium ova in urine samples. The Schistoscope uses a reversed lens attached to a smartphone or Raspberry Pi camera to magnify and take an image of an urine sample. An algorithm localizes and classifies potential ova. The SODOS uses an optical sensor and a lens to perform a holographic analysis of urine samples. The algorithm digitally reconstructs the image, from which ova are classified. These technologies can offer the following benefits compared to microscopy; 1) Simple and user friendly; 2) Rapid; 3) Sensitive; 4) Robust and portable; 5) Affordable; 6) Data collection.
An qualitative research with semi-structured interviews was conducted in Oyo State, Nigeria to explore the context and identify gaps and stakeholders for i) case management on primary healthcare level, and ii) the control & elimination program. The main problem in case management is that diagnosis is not done at primary level due to limited resources and awareness, which leads very few confirmed cases. For case management, the stakeholders are divided into healthcare enablers, formal health providers, informal health providers and healthcare receivers. The control & elimination program is divided into i) mapping of schistosomiasis prevalence and ii) mass drug administration during Deworming days. The problem in the control & elimination program is that lack of diagnosis leads to an unknown disease prevalence. As a result, there is limited government interest and funding. For the control & elimination program the stakeholders are divided into initiation, organization, mapping implementation, Deworming implementation and target populations. The benefits from technology were combined with gaps in the healthcare context into twelve opportunities for diagnostic scenarios. Three diagnostic scenarios were selected; 1) Test at PHC consult by a community health worker, which allows testing at PHC level; 2) Mapping of adult populations at risk, where adults are tested at occupational group meetings by community health worker and/or lab assistant; 3) Test as sensitization tool, where diagnosis is done by a community resource person in communities to create awareness. Insights from the research were combined into target product profiles with acceptable and ideal values for product attributes. A creative session was organized to determine the value of this specification list for product design.
Have a look at the full thesis report here.